Paul Tambyah criticises ISP rider changes, urges shift to single-payer healthcare model
SDP Chairman Paul Tambyah, in a Facebook video on 9 December, warned that new ISP rider rules could delay treatment and overwhelm public hospitals. He called for a universal healthcare financing model and criticised piecemeal reforms lacking transparency.

Singapore Democratic Party (SDP) Chairman Paul Tambyah has warned that upcoming changes to Integrated Shield Plan (ISP) riders could result in delays in early medical treatment and increased burden on public hospitals.
Tambyah made these comments in a video posted to his Facebook page on Tuesday, 9 December 2025, in his capacity as party chairman.
In addition to his political role, Tambyah is a Professor of Medicine at the National University of Singapore (NUS) and Senior Consultant in the Division of Infectious Diseases at the National University Hospital (NUH). He has held numerous academic and advisory appointments since the early 2000s, including with the Singapore Armed Forces, the Infectious Diseases Society of America, and the Western Pacific Society of Chemotherapy.
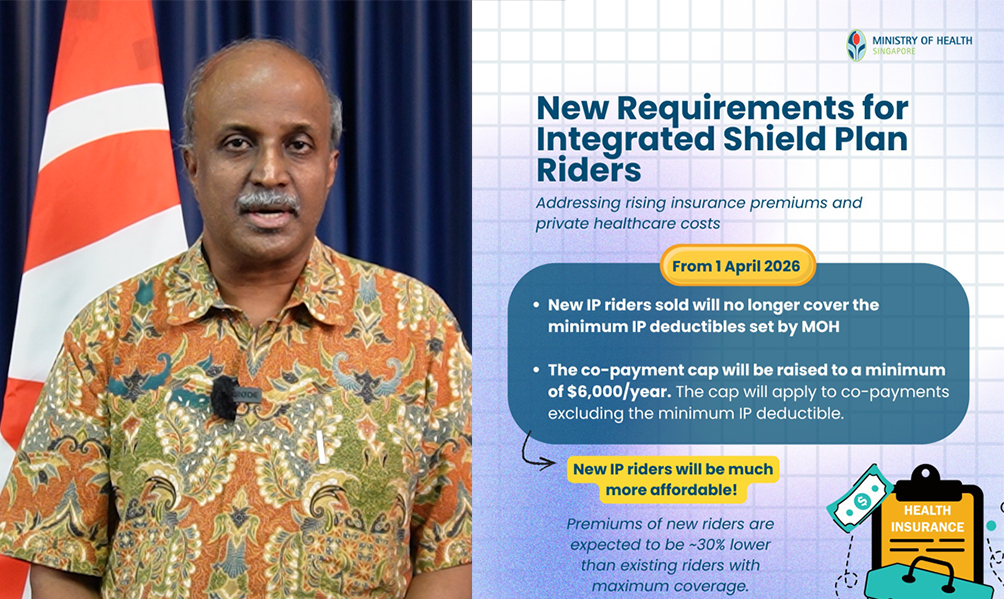
Under changes announced by the Ministry of Health (MOH) in November 2025, all new ISP riders sold from 1 April 2026 must exclude coverage of the mandatory deductible—ranging from S$1,500 to S$3,500 depending on ward class—and double the annual co-payment cap from S$3,000 to S$6,000 for eligible claims.
The MOH stated that these revisions aim to curb rising healthcare costs and restore insurance to its original role—protecting against high-cost events, rather than routine bills. The Ministry also projects that premiums for new private hospital riders could drop by around 30%.
However, Tambyah raised concerns that this structure may disincentivise patients from seeking timely care.
“There is a real fear that the co-payment of S$6,000 will discourage people from seeking essential treatment early,” he said, citing breast lump biopsies as an example where the cost could fall below the co-payment threshold.
Such deterrence, he argued, could lead to late-stage diagnoses and worse health outcomes. Tambyah described this as a “penny wise and pound foolish” approach, citing international and local research that links healthcare avoidance to high out-of-pocket costs.
He also criticised a case study from MOH’s press release involving a woman undergoing ACL reconstruction at a private hospital, who faces a S$1,360 co-payment even after Medisave deductions.
He questioned the omission of Medishield Life from the cost breakdown and asked: “Then pay Medishield Life premiums for what?”
Tambyah warned that the reforms could push more patients—particularly those who previously used riders to access private care—into public hospitals. “Public hospitals are likely to have to take over a large chunk of people who used to be able to go to private hospitals,” he said.
This, he argued, may create friction as former private patients accustomed to faster service confront longer wait times and emergency prioritisation in public hospitals.
Drawing on personal experience in the public sector, Tambyah said he has frequently had to calm A-class patients frustrated by delays, noting that public hospitals operate under different principles and resource constraints.
“These kinds of piecemeal adjustments to our healthcare financing system without underlying transparent data justifications could have significant adverse unintended consequences,” Tambyah said, calling for broader reform.
Tambyah concluded his remarks by reiterating the SDP’s longstanding call for systemic reform of Singapore’s healthcare financing model.
SDP’s alternative healthcare proposal
First introduced in 2019 and reaffirmed during the 2025 General Election, the SDP’s healthcare plan proposes a universal, single-payer insurance scheme to replace the current “3Ms” framework—Medisave, Medishield, and Medifund.
The proposal centres on the National Health Investment Fund (NHIF), which would provide coverage for basic health, accident, and pregnancy-related services for all Singaporeans and permanent residents residing in the country for at least six months a year.
Under the plan, every Singaporean would contribute S$50 monthly from their Central Provident Fund (CPF) accounts. The rest of the funding would come from general taxation. Patients would only need to co-pay 10% of their hospital bill, with an annual cap of S$2,000.
Tambyah described this approach as simpler and more equitable than the current system. “This payment from a single source rather than multiple sources from the 3Ms eliminates the present complicated subsidy system,” he said at a media briefing in May 2019.
He also pointed to historical precedent, noting that Singapore previously operated a single-payer model during the 1960s and 1970s, which he described as a “golden era” for healthcare outcomes and equity.
Criticising the commercialisation of public healthcare since the 1980s, Tambyah argued that treating health as a commodity has led to inequality and underinsurance. He cited data showing significant disparities in life expectancy between socioeconomic groups and observed that many avoid treatment due to cost—even when diagnosed with chronic conditions like hypertension.
“Healthcare is treated like a commodity where people avoid important primary healthcare services because of the costs and end up spending a lot of money treating complications that could have been prevented,” he said.
(First published on Heidoh)
Update on 12 Dec 2025:
Tambyah wrote:
"I’ve taken down my previous video on the friendly advice of an old friend (who almost fell asleep watching it).
Apparently some people may have misunderstood the original post to be about the CURRENT public healthcare system. It was actually expressing some concerns about what might happen (based on a review of the medical literature) if and when the co-payment cap for private insurance with riders is raised to $6000 on 1st April 2026.
There are still four months to go so you have time to optimise your Shield plan to make sure that you do not miss out on any essential procedures (just below $6K) in the private sector and do not stress our excellent public healthcare system.
Talk with your MP about the mitigation measures that the authorities have probably lined up to prevent any unintended adverse consequences from these changes.
Personally, I still think that we need a simpler, single payer universal healthcare system like the one proposed by the SDP."